Mandibular Fracture Repair
Case Report
Chloe Joslin 1343831
Veterinary Medical and Surgical Care NSCI 6100
04 August 2011
Abstract
A shallow oblique fracture of the rostral third of the left mandible was diagnosed in a dog following trauma sustained from other dogs. The repair procedure can be challenging where trauma to an artery, vein and nerve must be avoided but prognosis is good following use of correct technique. Stouts interdental wiring and acrylic was used successfully for the fracture repair done under general anaesthesia. Normal occlusion of the oral cavity was maintained. Acrylic and wire were removed after six week follow-up radiographs showed bony healing and the mandible was palpably stable.
Signalment
Name Roxy
Species Canine
Breed Bichon Frise
Age Estimated 7years 9 months
Sex Female (spayed)
Colour White
Weight 6.6kg
Body condition score 5/10
History
03 August
Roxy was attacked by two dogs and promptly presented to a referral clinic. There was bleeding from the mouth and two large puncture wounds over the thorax. There was no evidence that the chest wall was ruptured. An unstable fracture of the left mandible was identified.
Respiratory rate was within the normal species range of 10 to 30 breaths per minute (brpm) (Lane, Cooper & Turner, 2009, p.233). Temgesic 0.4millilitres (ml) was administered subcutaneously at 5.30pm, 8.00pm and 11.00pm. Cephalexin 1ml was given subcutaneously at 6pm. Cephalexin is part of the cephalosporin group of antibiotics. It destroys the bacterial cell wall killing the bacteria (“Cephalexin,” 2011). Cephalosporins have a low incidence of adverse effects (Bassert & McCurnin, 2010, p.837).
Lactated Ringers Solution (LRS) fluids were administered intravenously. Roxy was Anaesthetised with Alfaxan® (Alfaxalone), an injectable anaesthetic (Alfaxan, n.d.), and maintained on Isoflurane gas to enable assessment of the chest wound and mandible. A six inch incision was made between the thoracic bite wounds. Severely damaged skin and subcutaneous tissue was debrided from the ribs and muscles. The ribs and the thoracic wall are not damaged. A penrose drain which is a soft latex tube was placed inside the wound. This is a passive drain meaning that gravity and capillary action is relied upon to drain any accumulation of fluid within the wound (Lane, Cooper & Turner, 2009, p.605). The subcutaneous tissue was closed with 3/0 polydioxanone, an absorbable monofilament suture which consequently entails less tissue drag. The skin layer was sutured with 3/0 nylon, a nonabsorbable polymerized plastic suture (Bassert & McCurnin, 2010, p.1004).
Clinical Examination
04 August
Subjective assessment: Roxy is quiet but responsive. She is sitting up at the front of the kennel looking a little confused but does unfortunately have a few noisy neighbours in the dog ward today so she may be a little overwhelmed (VSG, personal communication, 5 august, 2011).
Objective assessment: Roxy’s rectal temperature measured 37.4°Centigrade (C) which is slightly lower than the normal temperature range of 38.3°C to 38.7°C. The heart rate was 110 beats per minute (bpm) which is within the normal range of 60 to 180 bpm (Lane, Cooper & Turner, 2009, p.233). The respiration rate without exertion was 30brpm which is not a concern. The mucous membranes were pink and the capilliary refill time (CRT) was less than two seconds which indicates peripheral perfusion of blood and therefore oxygen. Without oxygen tissue necrosis will occur. The fracture of the left mandible was noted rostral to the carnassial teeth which are the maxillary fourth premolar and the mandibular first molar teeth (see figure 1.); the largest shearing teeth (Bassert & McCurnin, 2010, p.1098).
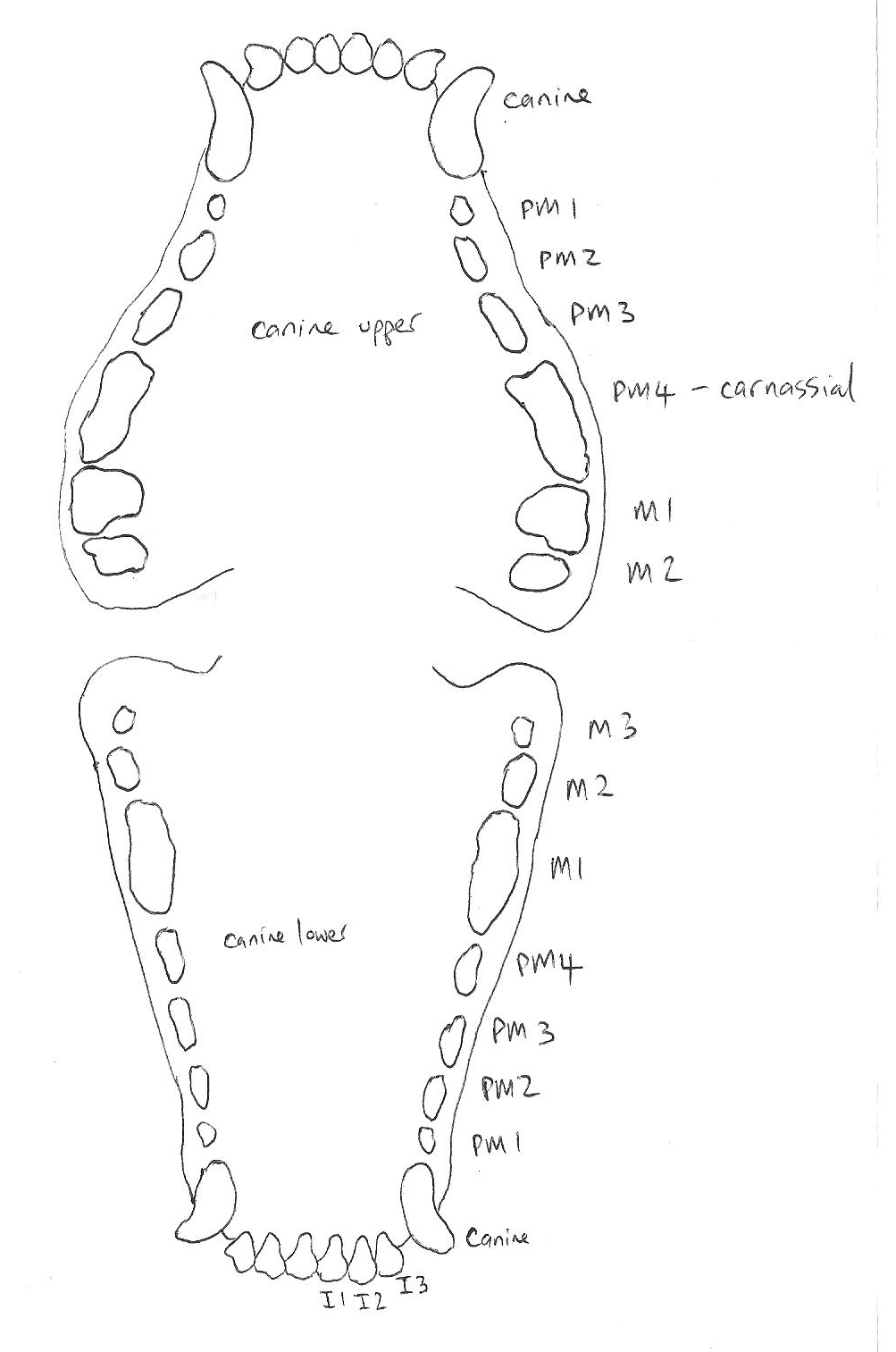
Figure 1. Canine tooth layout. Drawing: Chloe Joslin. Taken from Pfizer Animal Health chart.
Housing
Post operatively Roxy was initially placed into a fold-down wire cage to allow good observation, size 100cm long, 80cm wide, 80cm high. There must be enough room for comfortable lateral recumbency but restrictive to allow rest. This was placed away from direct sunlight and draughts. Bedding was made comfortable using towels, blankets and a vet bed designed to pull urine through the bed away from the patient preventing possible urine scald during recumbency. When continuous monitoring is no longer necessary, Roxy was moved to a slightly larger fibreglass cage in the kennel room. Fibreglass is easily maintained.
Diagnosis
Roxy is sedated and a radiograph of her thorax is taken, which is an advised procedure, following trauma to ensure no further internal damage has been endured. Five views are taken including dorsal-ventral, lateral right and left, oblique and intraoral (Fossum et al., 2000, p.639). The radiograph views reveal a shallow oblique fracture of the rostral third of the left mandible.
Bandaging of the mid to caudal thorax compromises image quality but a slight loss of radiolucency through the dorsal lung lobes is detected which may indicate and mild pulmonary contusion (similar to a bruise on the lung) (Lane, D. R., Guthrie, S., Griffith, S., 2008) which is a concurrent injury often present with fractures caused by head trauma (Fossum, 1997, p.767). See Radiograph below and appendix. Drooling and a reluctance to eat can signify a mandibular fracture but a general anaesthetic is necessary to enable a thorough examination to confirm this diagnosis (Fossum, 1997, p.767). A pre anaesthetic blood test would not show abnormalities due to the fracture but would ensure Roxy’s vital organs ability

Thoracic radiograph 4th August. (VSG 2011).
Condition
A mandibular fracture can be very challenging to immobilize long enough for healing to take place therefore thorough knowledge of mandibular anatomy and biomechanics is essential. There is an artery and vein, which are the only blood supply to mandibular teeth, running through the mandibular canal. This canal also contains an alveolar nerve. Trauma to these structures must be avoided during fracture reduction procedure (Jerram, 2011).
Prognosis
A procedure consent form has been signed by the owner outlining possible complications involved in the procedure. The prognosis of mandibular fracture repair is good if proper techniques of fracture management are carefully achieved. This includes the mandibular alveolar nerve, artery and vein not being damaged which does often happen and clinical signs are seldom seen. The oral cavity contains a high number of bacteria therefore prophylactic bacteria should be administered although infections are rare as vascular supply to the mandible is strong (Fossum, 1997, p.774).
Normal occlusion must be returned to the jaw although compensation can be learnt if malocclusion occurs (Fossum, 1997, p.768). Osteomyelitis (Inflammation of the bone caused by trauma) is treated with stabilization and appropriate antibiotics (Fossum, 1997, p.778).
Treatment Options
Radiograph viewing determines the exact treatment to be used for Roxy. The mandibular fracture can be reduced and stabilized using Stouts interdental wiring (see figure 2.) and acrylic (VSG, personal communication, 5 august, 2011). Mandibular plating and screws or external fixators can be an alternative option but these can disrupt neurovascular supply to the mandible and the tooth roots (Jerram, 2011). Tape muzzles can be fitted enabling drinking and eating of soft food for six weeks (Fossum, 1997, p.768). If proper realignment of the mandibular and maxilliary teeth, which closely interdigitate, cannot be achieved with an ET tube in place during fracture repair, then the ET tube can be placed through a pharyngotomy incision, allowing complete mouth closure and therefore good dental occlusion (Fossum, 1997, p.774). All options are discussed with the owner.

Figure 2. Interdental wires placed through mandibular bone to prevent wire from slipping (Fossum, 1997, p.770).
Actual Treatment
Roxy was placed in left lateral recumbency, due to the fracture being on the left mandible, for ease of access to the site. Teeth involved in fractures should not be removed unless they are loose. An oral examination outcome exposed the looseness of the second left mandibular molar. This was extracted and the defect was closed using 4/0 Monocryl absorbable suture. The second right mandibular molar was also discovered to be slightly loose but was left in place.
The fracture was reduced and stabilized. Mucosa edges were debrided and apposed over the site using 4/0 Monocryl. Stouts interdental wiring was used as initial stabilization of the fracture with 25 gauge orthopaedic wire. The wire was placed on the teeth adjacent to the fracture lines and secured in the bone around the neck of the teeth to prevent movement. It is best to include two teeth either side of the fracture (Jerram, 2011).
Guide holes are drilled between teeth and through the superficial cortical bone surface. Wire is then passed through a 22 gauge needle which is inserted through the guide holes, circled around the teeth and tightened. The wire ends are bent into the mucosa (Fossum, p 640).
The left mandibular coronal (top) surfaces of the canine, premolars and first molar were acid etched with a 40% phosphoric acid gel and then rinsed. The acid etching creates micropores in the enamel that allow the acrylic to penetrate the enamel and bond to the teeth (Jerram, 2011). A self-curing dental acrylic was applied over the wire and teeth using an applicator gun. The buccal surface of the first molar was avoided. As the acrylic was hardening, the fracture was held in position to ensure the achievement of good stability and occlusion. Post operative radiographs confirmed good reduction and alignment. See radiograph below and appendix.

Stouts interdental wiring is used as initial stabilization of the fracture with 25 gauge orthopaedic wire. Photo: Chloe Joslin

Radiograph of Mandible 5th August showing Stouts interdental wiring. (VSG, 2011)
Fluid and Pain Management
04 August
Temgesic (Buprenorphine) of 0.3mg per ml (mg/ml) concentration was administered subcutaneously as pre emptive analgesia. Buprenorphine is a partial mu (opioid receptor (Tian, 1997)) agonist where dissociation from receptors is slower which provides a longer duration of analgesia lasting six to eight hours which is longer than morphine. The dose rate was 0.015 milligrams (mg) per kilogram (kg) body weight of the patient. The total dose of 0.33ml was administered at 3.00pm and then 10.00pm.
LRS intravenous fluids were administered at a maintenance rate of 16ml per hour (ml/hr). The drip rate used being 60 drops per second (dps). LRS fluid is alkalinizing; it contains lactate that is metabolized by the liver to form bicarbonate. Bicarbonate is a chemical (buffer) that keeps the pH of blood from becoming too acidic or too basic (“Carbon Dioxide (Bicarbonate),” 2010). LRS replaces water and electrolyte losses maintaining hydration (Lane, Cooper & Turner, 2009, p.401).
05 August
0.33ml Temgesic was administered at 5am. Morphine of 30mg/ml concentration was administered subcutaneously as analgesia. The dose rate was 0.6mg/kg and the dose given was 0.13ml. Morphine was administered one hour post surgery at 1.00pm and continued at six hour intervals as the duration of effect is four to six hours.
The patient was not eating or drinking post surgery so LRS intravenous fluids continued to be administered at a new maintenance rate of 14ml/hr using a drip rate of 50dps.
06 August
Temgesic was started again from 12.00pm and continued 0.33ml seven hourly. Metacam® (Meloxicam) is advised to be administered when Roxy starts eating which she did not start today. Metacam® is a NSAID (non-steroidal anti-inflammatory drug) (Brooks, 2011).
07 August
Temgesic was stopped following an assessment of being non-painful. Metacam® was administered once daily (SID) at 8.00am.
Nursing Care
04 August
The intravenous catheter, which was inserted by the referral clinic in the right cephalic vein, was flushed and found to be still patent. Roxy was walked outside at regular intervals. Fresh air provides good mental stimulation and encourages natural urination and defecation. Approximately 100ml a/d and water slurry was offered. Fresh water was also offered. Food was removed at 10.00pm in preparation for surgery the next day. The stomach must be almost empty as the premedication may induce vomiting which may cause aspiration of food down the trachea.
05 August
Prior to surgery Roxy was walked outside to urinate and defecate. A premedication of Atropine 0.022mg/kg, concentration 0.65mg/ml, total dose 0.2ml; Morphine 0.4mg/kg, concentration 5mg/ml, total dose 0.5ml; and Valium (Diazepam) 0.25mg/kg, concentration 5mg/ml, total dose 0.3ml are all administered subcutaneously. Atropine counteracts parasympathetic activity of the nervous system for example bradycardia and excess salivation; therefore increases the heart rate, decreases salivation and gastrointestinal activity and dilates the pupils (Bassert & McCurnin, 2010, p.891) Morphine is an opioid agonist with rapid onset of action used to provide analgesia and sedation. Side effects are minimal consisting of hypotension and vomiting. (Bassert & McCurnin, 2010, p.869). Diazepam is a Benzodiazepam tranquilizer which has an anti-anxiety effect with mild sedation; muscle relaxation and anticonvulsant with duration of a few hours maximum (Bassert & McCurnin, 2010, p.892). Roxy is monitored for any side effect onset.
At 10.00am Propofol (Diprivan) 4mg/kg, concentration 100mg/ml, total dose 2.6ml was administered intravenously to induct Roxy into anaesthesia. Propofol has rapid onset of 30 to 60 seconds and approximately two to five minute duration. Side effects are reduced intracranial and intraocular pressure, anti-emetic and anti-convulsant; initially apnoea can occur (Bassert & McCurnin, 2010, p.894). Then Roxy was intubated, the cuff inflated to seal the trachea and the endotracheal tube connected with a non-rebreathing circuit, to the anaesthetic machine providing oxygen and isoflurane anaesthetic agent. The pulse oximeter is attached to the tongue and the ultra sonic doppler cuff measured and attached to the carpal indicating systolic blood pressure.
Monitoring of pulse, heart, respiration rates and oxygen saturation were started and recorded at five minute intervals on a monitoring sheet (see appendix). The heart (180bpm) and respiration (97brpm) rates were very high at the beginning of anaesthesia during painful fracture reduction. For the remainder of the procedure the heart rate averaged 115bpm; the respiration rate ranged between 13 and 30brpm. 30brpm is high during anaesthesia indicating shallow depth and pain onset. Normal dog anaesthesia range is 8 to 20brpm (Bassert & McCurnin, 2010, Tables p.912). Saturation of peripheral oxygen, measured through the tongue pulse oximeter probe, remained approximately 98 as the average pulse rate and oxygen saturation in the blood. Anaesthesia was maintained on 2.5% isoflurane for most of the procedure with 2 litres per minute oxygen. LRS intravenous fluids were administered at a surgical rate of 66ml/hr. Mucous membranes remained pink and capillary refill time less than two seconds throughout. The eyes moved into ventral medial position 15 minutes into the procedure and returned twice to the central position indicating changes in depth of anaesthesia. The temperature was measured with a rectal thermometer every 30 minutes and remained at 36.6°C; normal during anaesthesia. 12.00pm end of procedure noted when the isoflurane gas is turned off.
Careful monitoring of vital parameters continued post operatively, with Roxy wrapped in a blanket, until the cough reflex was imminent and then the endotracheal tube cuff was deflated and Roxy was extubated. Nothing abnormal was detected and monitoring then continued at ten minute intervals until sternal recumbency was achieved and Roxy was fully awake.
1.32ml of Baytril® (active ingredient: enrofloxacin), an antibiotic, was administered subcutaneously. Baytril was given SID one hour post surgery at 1.00pm. Kefzol of 22mg/kg concentration was administered by slow intravenous infusion. The dose given was 1.5ml and is administered once at 10.00am then 12.00pm immediately post surgery then every eight hours (Q8). Kefzol (cephazolin) is a first-generation cephalosporin antibiotic. The bladder was manually expressed at 1.00pm post surgery. The bed was checked at 4.00pm and was dry. The owner is contacted with a post operative and radiographic findings update.
06 August
The staff at the after-hours clinic reported that Roxy was comfortable over the night. Morphine (0.5ml) was administered subcutaneously and Kefzol intravenously. LRS was continued as maintenance fluids overnight and will continue today until Roxy is eating. Temgesic was started subcutaneously. Baytril 50mg/tablet was administered at a dose of half a tablet per oral (PO) SID at 5.00pm. Clavulox, reliable broad spectrum antibiotics (Clavulox Palatable Tablets, 2008), 250mg/kg was administered at a dose of half a tablet PO twice (BID) at 8.00am and 5.00pm.
All physical parameters are within the normal range for Roxy. Slightly inappetant but drinking adequately. Walking outside to the toilet without differiculty.
The chest bandage is unwrapped to check the indwelling penrose drain which is still producing a moderate amount of discharge therefore it is decided to leave the drain in place and recheck tomorrow. The wound is recovered with TelfaTM antimicrobial dressing and swabs. Cast padding providing comfort, VetrapTM self-adherent bandaging and elastoplast conforming bandage are used to rebandage the chest.
Roxy was offered Hills® a/d in the form of watery slurry and she was interested in eating. Hills a/d offers good nutritional support for trauma recovery (“Prescription Diet® a/d® Canine/Feline Critical Care,” 2011).
The IV catheter was removed as patency was lost. The veterinary surgeon advised hospital care for another two days unless there was large improvement. The owner is called with an update on recovery.

Pulse oximeter placed on the tongue. The mandibular fracture visible. Photo: Chloe Joslin
07 August
Roxy is alert and responsive. All physical parameters are still within the normal range. Oral medications are pilled. Syringe fed 30mls a/d this morning and afternoon. The chest is unbandaged and with the drain producing only a small amount of discharge, it was removed and the chest rebandaged. One Baytril dose was administered at 3.00pm. Clavulox was administered at 8.00am and 3.00pm. The owner is called with another update in progress and the plan is for Roxy to go home tomorrow which will be confirmed in the morning.
08 August
Roxy is well improved today. Disinterested in eating but happy to be syringe fed. (VSG, personal communication, 5 august, 2011).
Discharge, After Care and Follow-Up
08 August
The client is advised to offer Roxy a soft food diet for the next six weeks to enable fast and accurate healing and ease of eating and there should be no running or strenuous exercise. After this period normal activity can return gradually. It is recommended that Roxy is taken to the referral clinic for a bandage change and wound assessment in two days. The sutures over that wound should be removed about the 14th of August. This would be ten days following the placement of the sutures which has given the wound adequate healing time. If there is any chest discharge over the bandage, any swelling, pain, vomiting, diarrhoea, inappetance or blood in the faeces then the medication should be discontinued immediately and VSG or the regular vet should be contacted without hesitation. The prescribed medication should be given as directed. A recheck is advised in six weeks for radiographs to be taken to check the healing progress and the acrylic and wire to be removed.
19 September
Roxy was admitted for a radiograph check of the left mandible, wire and acrylic splint removal, tooth extraction and a dental scale and polish. Roxy was premedicated with Atropine 0.22mls, morphine 30mg/ml concentration 0.06mls and Diazepam 0.33mls and induced with Propofol 2.6mls and maintained on mostly 2% Isoflurane without complication.
Radiographs showed some bony healing therefore the acrylic and wire were both removed using a dental burr, wire cutters and extraction forceps (Jerram, 2007). See Radiograph below and appendix. The mandible was palpably stable. The teeth cleaned and the loose molar two and left first incisor were removed. Post operative check was necessary to evaluate irreversible damage and the definite need for extraction (Fossum, 1997, p.767).
Recovery went well although very hypothermic post procedure at a temperature of 34.6°C. A bair hugger was placed and due to small body size the temperature raised to normal range within an hour. Temgesic is administered subcutaneously.
Clavulox tablets will need to be administered for five days. The owner is advised to offer a soft food diet for the next two to three weeks. Return to a normal diet should be possible after this period. No further rechecks should be necessary.


Radiograph of Mandible showing bony healing 19th September. (VSG, 2011)
Discussion
A common place for mandibular fractures in dogs is between the first premolar and second molar. Interestingly the second left molar was loosened due to the fracture which then needed extraction.
It is often read that the use of a tape muzzles can be used for stabilization during fracture repair but complications often occur (Jerram, 2011).
The use of external skeletal fixation, being the other method of possible repair, was avoided in this procedure as these can disrupt the vein, artery and alveolar nerve within the mandibular canal and also the tooth roots (Jerram, 2011). The procedure of interdental wire and acrylic used in this procedure has been successful a number of times and was again successful with Roxy in maintaining normal occlusion of the oral cavity.

Fracture repair with acrylic. (“Dental photos”, n.d.)
Acknowledgments
Thankyou to all the staff at VSG for the information they provided and the assistance they gave. I was encouraged to ask questions and all were readily answered.
Appendix



Thoracic radiograph 4th August. (VSG 2011).

Radiograph of Mandible 5th August showing Stouts interdental wiring. (VSG, 2011)

Radiograph of Mandible 5th August showing Stouts interdental wiring. (VSG, 2011)

Radiograph of Mandible 5th August showing Stouts interdental wiring. (VSG, 2011)

Radiograph of Mandible showing bony healing 19th September. (VSG, 2011)
References
Alfaxan. (n.d.). Retrieved from: http://www.alfaxan.com/#
Bassert, J. M., McCurnin, D. M. (2010). Clinical textbook for veterinary technicians. Missouri: Elsevier Limited.
Brooks, W. C., (2011) Meloxicam (Metacam). Retrieved from: http://www.veterinarypartner.com/Content.plx?P=A&A=1752
Carbon Dioxide (Bicarbonate). (2010). Retrieved from: http://www.webmd.com/a-to-z-guides/bicarbonate
Cephalexin. (2009). Retrieved from: http://www.drugs.com/cephalexin.html
Clavulox Palatable Tablets. (2008). Retrieved from: http://www.pfizeranimalhealth.co.nz/sites/pfizeranimalhealth/Pages/ClavuloxPalatableTablets.aspx?Species=Cats
Dental photos. (n.d.). Retrieved from: http://allpetsdentalcare.com/dentalphotos.html
Fossum, T. W., (1997). Small animal surgery. Missouri: Mosby, Incorporated.
Fossum, T. W., Hedlund, C. S., Hulse, D. A., Johnson, A. L., Seim, H. B., Willard, M. D. & Carroll, G. L. (2000). Manual of small animal surgery. Missouri: Mosby, Incorporated.
Jerram, R. (2011). Lecture presented at Unitec Institute of Technology, Auckland, New Zealand.
Jerram, R., (2007). Plastic Fantastic Orthopaedics. Retrieved from: http://www.vsg.co.nz/documents/vsgnews09.pdf
Lane, D., Cooper, B., Turner, L. (2009). BSAVA textbook of veterinary nursing, (4th ed.). Glouster: British Small Animal Veterinary Association.
Lane, D. R., Guthrie, S., Griffith, S. (2008). Dictionary of veterinary nursing, (3rd ed.). Philadelphia: Elsevier Limited.
Prescription Diet® a/d® Canine/Feline Critical Care. (2011). Retrieved from: http://www.hillspet.com/products/pd-feline-ad-caninefeline-critical-care-canned.html